
From the 1Department of Rehabilitation and 3Department of Rehabilitation Medicine, Tokyo Shinjuku Medical Center, Japan Community Health care Organization, and 2Graduate School of Comprehensive Human Sciences, University of Tsukuba, Tokyo, Japan
Objective: To investigate the impact of unilateral spatial neglect with or without other cognitive impairments on recovery of independent gait in stroke survivors.
Design: A prospective cohort study.
Subjects: Ninety-four stroke survivors in an inpatient rehabilitation ward.
Methods: The presence of unilateral spatial neglect was assessed by the visuospatial perception score of the Stroke Impairment Assessment Set, and other cognitive impairments were assessed by Mini-Mental State Examination. Participants were categorized into 3 groups: group 1, unilateral spatial neglect with other cognitive impairments; group 2, unilateral spatial neglect without other cognitive impairments; and group 3, non-unilateral spatial neglect. The outcome was the walking score of the Functional Independence Measure (FIM) at discharge (score ≥ 6 or ≤ 5).
Results: Multivariate logistic regression analysis (reference, group 3) showed that the presence of unilateral spatial neglect with other cognitive impairments (group 1) had a significant association with dependence of gait (p = 0.003), and the odds ratio (95% confidence interval) was 5.55 (1.19–23.04). In contrast, there was no significant relationship between the presence of unilateral spatial neglect without other cognitive impairments (group 2) and dependence of gait (p = 0.207).
Conclusion: The presence of unilateral spatial neglect without other cognitive impairments is not a significant factor for regaining independent gait. In contrast, unilateral spatial neglect becomes a strong negative factor when combined with other cognitive impairments.
Key words: stroke; hemispatial neglect; cognitive impairment; gait.
Accepted Oct 8, 2018; Epub ahead of print Nov 8, 2018
J Rehabil Med 2019: 51: 00–00
Correspondence address: Yosuke Kimura, Department of Rehabilitation, Tokyo Shinjuku Medical Center, Japan Community Health care Organization, 5-1 Tukudocho, Shinjuku-ku, Tokyo 162-8543, Japan. E-mail: mcbb10ver@yahoo.co.jp
Unilateral spatial neglect is characterized by reduced awareness of stimuli on one side of the body. Spatial neglect is a common cognitive impairment in stroke patients with damage to the right side of their brain. In addition, stroke often causes other cognitive impairments, such as memory deficits and non-spatial attention deficits. These neurological symptoms may affect recovery from stroke. This study investigated whether the presence of spatial neglect in combination with -other cognitive impairments negatively affects the recovery of gait ability in stroke patients. It was found that, in the absence of other cognitive impairments, spatial neglect did not have a negative impact on recovery of gait ability. In contrast, if associated with other cognitive impairments, spatial neglect was found to exacerbate recovery. This information will be helpful in developing optimal rehabilitation programmes for the recovery of gait ability in stroke patients.
R
ecovery of independent gait is one of the main goals in rehabilitation of stroke survivors (1). Independence of gait in stroke survivors is associated with ability to perform activities of daily living (ADL) (2), quality of life (3), caregiver burden (4), discharge destination (5) and even prognosis of survival (6). Therefore, it is important to investigate the factors associated with recovery of independent gait in order to develop optimal rehabilitation programmes and discharge plans.
Unilateral spatial neglect (USN) is thought to play a crucial role in the functional disadvantages in stroke survivors. USN leads to significantly poorer recovery of ADL ability (7, 8) and gait dependency (9, 10). However, other previous studies have indicated that the improvement in ADL ability does not differ according to the presence or absence of USN (11), and that the recovery of independent gait is not affected by the severity of USN after controlling for the severity of paresis (12). In addition, relatively recent studies have reported that there are no significant relationships between USN and ability in independent gait in outdoor settings, in chronic stroke survivors (13, 14). Thus, the association between USN and recovery of gait independence remains controversial.
Other cognitive impairments (CIs), such as memory deficits and non-spatial attention deficits, are common symptoms in stroke survivors, and they negatively influence their functional outcome (15, 16). In addition, previous studies have reported that, compared with stroke survivors without USN, those with USN are more likely to have other cognitive dysfunctions (17, 18). Thus, it is important to consider other cognitive functions in addition to USN in the prediction of gait ability in stroke survivors.
The Mini-Mental State Examination (MMSE) is an easily applicable and most widely used instrument in screening for CIs in stroke survivors. Several studies have reported acceptable validity of the MMSE as a screening tool and its relationship with functional recovery in stroke survivors (19–21). In addition, another previous study reported that the MMSE score reflects the number of disturbed cognitive domains, such as memory, mental speed, and non-spatial attention, in subacute stroke survivors (22). Although the value of the MMSE in screening for cognitive dysfunctions in stroke survivors remains controversial (23), it is considered a useful indicator for conveniently evaluating other cognitive dysfunctions.
This study aimed to investigate the impact of USN with or without other CIs on the recovery of independent gait in subacute stroke survivors. We hypothesized that the presence of USN without other CIs would be less negatively associated with the recovery of independent gait, and that it might be a strong negative factor when combined with other CIs. Clarification of these relationships would help in considering the prognostic prediction and interventions for regaining independent gait.
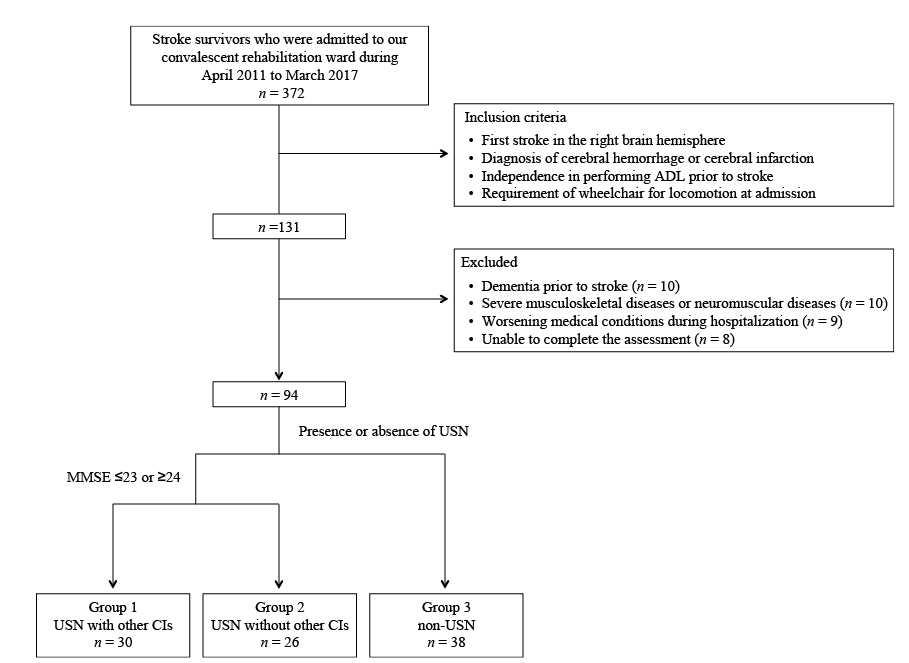
This prospective cohort study was conducted on stroke survivors admitted to the 37-bed convalescent inpatient rehabilitation ward of our hospital from April 2011 to March 2017. Diagnosis of stroke was based on clinical examination by a physiatrist and an imaging test (computed tomography or magnetic resonance imaging) by a radiologist. Inclusion criteria were: first stroke in the right brain hemisphere; diagnosis of cerebral haemorrhage or cerebral infarction; independence in performing ADL prior to stroke; and requirement for a wheelchair for locomotion on admission. Exclusion criteria were: presence of neuromuscular diseases or severe musculoskeletal diseases, worsening medical conditions during hospitalization (such as a recurrence of stroke or severe infection that would contraindicate rehabilitation), and inability to complete the assessment. In addition, participants who had a diagnosis of dementia prior to stroke, and those who had a pharmacological intervention on cognitive impairments prior to stroke were excluded. The study was conducted in accordance with the principles of the Declaration of Helsinki, and it was reviewed and approved by the ethics committees of our hospital (approval number: 27–20).
The presence of USN was assessed by the visuospatial perception score of the Stroke Impairment Assessment Set (SIAS) (24). The visuospatial perception score of the SIAS was evaluated on admission and at discharge. A 50-cm long tape measure was used for evaluation, and the central point method was adopted. Participants were asked to touch the midpoint of a tape held horizontally 50 cm in front of them, using the unaffected thumb and index finger. Two trials were allowed, and the worst error was used for the scoring value. If there was more than a 15-cm deviation from the midpoint, the score was 0. An error between 15 cm and 5 cm was scored as 1, while an error between 5 cm and 2 cm was scored as 2. A score of 3 meant deviation from the midpoint by less than 2 cm. We defined the presence of USN as a visuospatial perception score of 2 or less. This method was confirmed to have good inter-rater reliability and concurrent validity, assessed via 20-cm line bisection and flower-and-cube copying tasks in stroke survivors (24).
Other cognitive functions were assessed on admission by using the MMSE, which consists of the following 5 areas of cognitive functions: orientation, memory, attention and calculation, language, and construction. The total scores vary from 0 to 30, with higher scores indicating better cognitive functions. In this study, other CIs were defined as a score of less than 24 in the MMSE (the cut-off value was defined by referring to previous studies) (10, 21).
We investigated the gait dependency of the participants upon discharge, with the walking score of the Functional Independence Measure (FIM) (25) as the outcome measure. A FIM walking score of 7 corresponds to complete independence, wherein the participant can safely walk a minimum of 150 ft (50 m) without using assistive devices. A FIM walking score of 6 corresponds to modified independence, wherein the participant can walk a minimum of 150 ft (50 m) without supervision, but with the support of a brace (orthosis) or cane. FIM walking scores of 1–5 correspond to requiring help or supervision and are determined by the level of physical assistance required for walking. In this study, gait independence was defined as a FIM walking score of 6 or more, according to a previous study (26).
Demographic characteristics and stroke-related information including age, sex, stroke type (cerebral infarction or cerebral haemorrhage), number of days from onset of stroke to admission, length of stay, body mass index, comorbidity, use of medication (antidepressants and anxiolytics), severity of hemiplegia of the lower limb, and ability to perform ADL were investigated on admission to our rehabilitation ward. Comorbidity was assessed using the Charlson comorbidity index (CCI) (27). The CCI is an evaluation index with 1 to 6 points for 19 comorbidities, with a higher score indicating greater comorbidity. The severity of hemiplegia was determined in terms of the Brunnstrom recovery stages (BRS) (28). The BRS classifies voluntariness in paralysed limbs into 6 ordinal stages, with the lower stages indicating severe paralysis. ADL ability was assessed using the FIM. The FIM is composed of 18 items divided into 6 subcategories: self-care (6 items), sphincter control (2 items), transfers (3 items), locomotion (2 items), communication (2 items), and social cognition (3 items). Each item is scored on a 7-point ordinal scale from a score of 1 (total dependence) to 7 (complete independence). The high reliability of the FIM for stroke survivors has been reported previously (25).
In the Japanese medical insurance system, participants are referred from acute hospitals approximately 30 days after onset of stroke and receive hospital care in convalescent rehabilitation wards for up to 180 days (29). In this study, all participants underwent rehabilitation programmes every day during hospitalization. The programmes were based on a comprehensive approach and included physical, occupational, and speech therapies, as necessary. Participants were provided with approximately 2 h (median 118 (interquartile range (IQR) 100–136) min) of rehabilitation programmes per day. There was no specific protocol or procedure for treating USN in this study. All participants with USN underwent approximately equivalent amounts of conventional therapies, such as visual scanning training, trunk rotation training, and feedback training in ADL tasks. In addition, participants with other CIs underwent conventional cognitive training.
The participants were assigned to 3 groups according to the presence or absence of USN and the MMSE score on admission: group 1, USN with other CIs; group 2, USN without other CIs; and group 3, non-USN (Fig. 1).
The characteristics of the participants were compared across the groups by 1-way analysis of variance, Kruskal–Wallis test, χ2 test, and Fisher’s exact test after evaluating the normality of the variables using the Shapiro–Wilk test. To examine the effect of the USN and other CIs on recovery of independent gait, we used logistic regression analysis using the 3 groups as the independent variables (reference, group 3) and the FIM walking score (score ≥ 6 or ≤ 5) as the dependent variables. In the logistic regression analysis, 2 models were used. In the first model, we did not adjust for covariates (Model 1, Crude); in the second model, in addition to Model 1, variables with p < 0.05 in univariate analysis were included as covariates (Model 2, multivariate model).
Statistical significance was defined as a p-value less than 0.05 for all analyses. Statistical analyses were performed using the SPSS software version 24.0 (IBM, Tokyo, Japan).
During the study period, 131 consecutive stroke survivors met the inclusion criteria, and 94 were analysed in the present study (Fig. 1).
Fig. 1. Flow chart of the participants’ selection process. USN: unilateral spatial neglect; CIs: cognitive impairments; MMSE: Mini-Mental State Examination.
The characteristics of the participants are shown in Table I. The mean age of the study participants was 69.9 years ± 9.3, and 57 (62.8%) were men. A total of 44 participants (46.8%) had had an ischaemic stroke and 50 (53.2%) had had a haemorrhagic stroke. Group 1 (USN with other CIs) consisted of 30 participants (31.9%); group 2 (USN without other CI), 26 participants (27.7%); and group 3 (non-USN), 38 participants (40.4%). With regard to baseline characteristics, significant differences in the length of stay (p = 0.002), BRS of the lower limb (p = 0.033), and FIM scores on admission (p < 0.001) were observed among the 3 groups. The prevalence of USN at discharge was 76.7% (n = 23) in group 1 and 53.8% (n = 14) in group 2 (p = 0.072). The frequency of regaining independent gait upon discharge was 35.1% (n = 33) overall, 10.0% (n = 3) in group 1, 50.0% (n = 13) in group 2, and 44.7% (n = 17) in group 3 (p < 0.001).
Table I. Characteristics of the participants
The results of the logistic regression analysis for the 3 groups (reference, group 3) in regaining independent gait are shown in Table II. In Model 1 (Crude model), the presence of USN with other CIs (group 1) showed a significant association with dependence of gait upon discharge (p = 0.004), and the odds ratio (OR) (95% confidence interval (95% CI)) for dependence of gait was 7.29 (1.18–28.20). In contrast, there was a non-significant relationship between the presence of USN without other CIs (group 2) and dependence of gait at discharge (p = 0.679). After adjustment for covariates (Model 2), the presence of USN with other CIs (group 1) still showed a significant association with dependence of gait (p = 0.003), and the OR (95% CI) for dependence of gait was 5.55 (1.19–23.04). There was a non-significant relationship between the presence of USN without other CIs (group 2) and dependence of gait at discharge (p = 0.207).
Table II. Logistic regression analysis for dependence of gait at discharge.
Right hemisphere stroke survivors were assigned to 3 groups based on the presence or absence of USN and on MMSE score at admission to the convalescent inpatient rehabilitation ward and their association with recovery of independent gait was investigated. The results showed that the presence of USN without other CIs (group 2) was not significantly related to recovery of independent gait during hospitalization. However, the presence of USN with other CIs (group 1) had a significant negative impact on the recovery of independent gait, even after adjustment for covariates such as age, motor-FIM score on admission, and severity of hemiplegia of the lower limb. Thus, the presence of USN becomes a strong negative predictor of independent gait recovery when combined with other cognitive dysfunctions.
These results showed that USN was not significantly associated with recovery of independent gait in stroke survivors without other CIs. This result is consistent with some previous studies, which showed that USN had no negative prognostic influence on gait ability and ADL ability (12, 30). Several previous studies have investigated the time course of USN recovery and shown that the severity of neglect greatly improved until about 12 weeks after the onset of stroke (31–33). Another recent study reported that the improvement in the severity of neglect significantly correlated with increased MMSE scores in subacute stroke survivors (34). In our results also, neglect symptoms disappeared at discharge in approximately half of the stroke survivors in group 2. Therefore, the influence of the presence of USN at admission on independent gait recovery might be limited in stroke survivors with relatively good other cognitive functions. In contrast, approximately 75% of stroke survivors in group 1 still had neglect symptoms at discharge and were significantly inhibited from regaining independent gait.
Several studies have concluded that USN is a negative predictive factor of functional outcome in stroke survivors (7–10, 34, 35). Unlike these previous studies, our results showed that USN was not significantly associated with recovery of independent gait in stroke survivors without other CIs. Stroke survivors with USN often have other cognitive dysfunctions that negatively influence functional recovery. However, some of the previous studies that concluded USN as a negative predictive factor of functional outcome did not consider other cognitive functions (7, 34, 35), in other words, whether USN itself or its combination with other CIs played a crucial role in functional recovery is unclear. The influence of USN may be overestimated unless other cognitive functions are considered.
The main finding of this study is that the presence of USN with other CIs had a strong negative impact on recovery of independent gait. Stroke survivors with USN are unable to orient their attention toward the left hemi-space and often are not aware of the left side of their body while performing everyday tasks. These neglect symptoms could lead to unstable walking, for instance, because stroke survivors with spatial neglect tend to bump into objects (36). Awareness regarding disability is a key determinant to overcoming these neglect symptoms in stroke survivors with USN (37). Cognitive skills, such as short-term verbal memory, non-spatial attention, comprehension, and orientation, are fundamental to the awareness and understanding of the impairments, as well as understanding the relationship between insight and the capacity to learn. Deficits in these cognitive skills could interfere with stroke survivors’ awareness of neglect symptoms and inhibit learning of compensatory strategies to overcome disabilities in the rehabilitation and ADL settings. Therefore, the presence of USN with a low MMSE score may have a strongly negative impact on recovery of independent gait in stroke survivors.
This study has several limitations. First, the subtypes of USN were not considered. A previous study reported that the improvement in ADL differed depending on the subtypes of USN (38), and that it could also be associated with gait independence. Therefore, it is necessary to consider a more nuanced definition of USN in future studies. Secondly, the sample size was relatively small; in particular, only 3 participants in group 1 regained independent gait. Further studies will require a larger cohort and the inclusion of stroke survivors with various severities. Thirdly, we did not examine the more detailed domains of cognitive functions, such as memory, language, attention, and executive function. Further studies are warranted to investigate the relationships between specific domains of cognitive impairment and functional outcomes. Finally, we did not investigate information regarding apathy and anosognosia for hemiplegia. Apathy and anosognosia are often found in stroke survivors and are known to have a negative effect on functional outcome (30, 39, 40). Further studies should investigate these symptoms and take into account their influence on the recovery of gait ability in stroke survivors.
The presence of USN in subacute stroke survivors with relatively good other cognitive functions was not significantly associated with recovery of independent gait during hospitalization in the convalescent rehabilitation ward. In contrast, stroke survivors with USN and other CIs were significantly inhibited from regaining independent gait even after controlling for covariates such as ADL ability at admission, and severity of hemiplegia. These findings indicated that USN became a strong negative predictor when combined with other cognitive dysfunctions, and that only 10% of the stroke survivors with both USN and other CIs regained independent gait during hospitalization. These results may be helpful in accurate prediction of the prognosis of subacute stroke and decisions regarding interventions required for recovery of independent gait in subacute stroke survivors.
We thank the nursing staff and rehabilitation therapists of JCHO Tokyo Shinjuku Medical Center for their contributions to the data collection.
We are also grateful to our laboratory members and Ms Mai Kawamura for their helpful advice on drafts of this manuscript.


 Click to show fullsize
Click to show fullsize Click to show fullsize
Click to show fullsize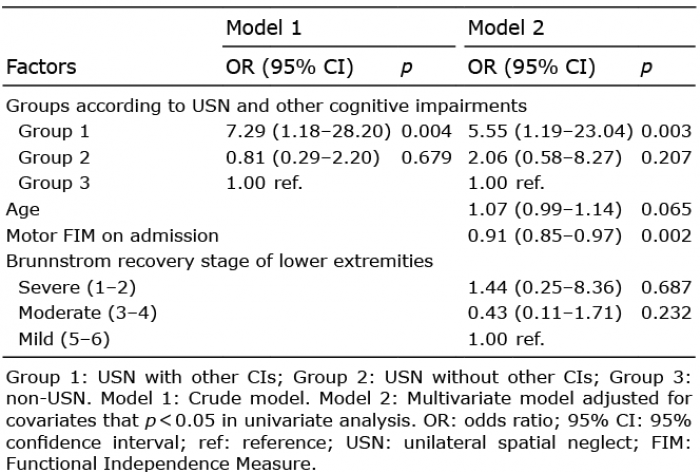 Click to show fullsize
Click to show fullsize